User login
Language
Anonymous's groups in this site
User is not a member of any group.
Your groups across all your sites
User is not a member of any group.
Recent Content
Who's online
There are currently 0 users online.

User is not a member of any group.
User is not a member of any group.
There are currently 0 users online.
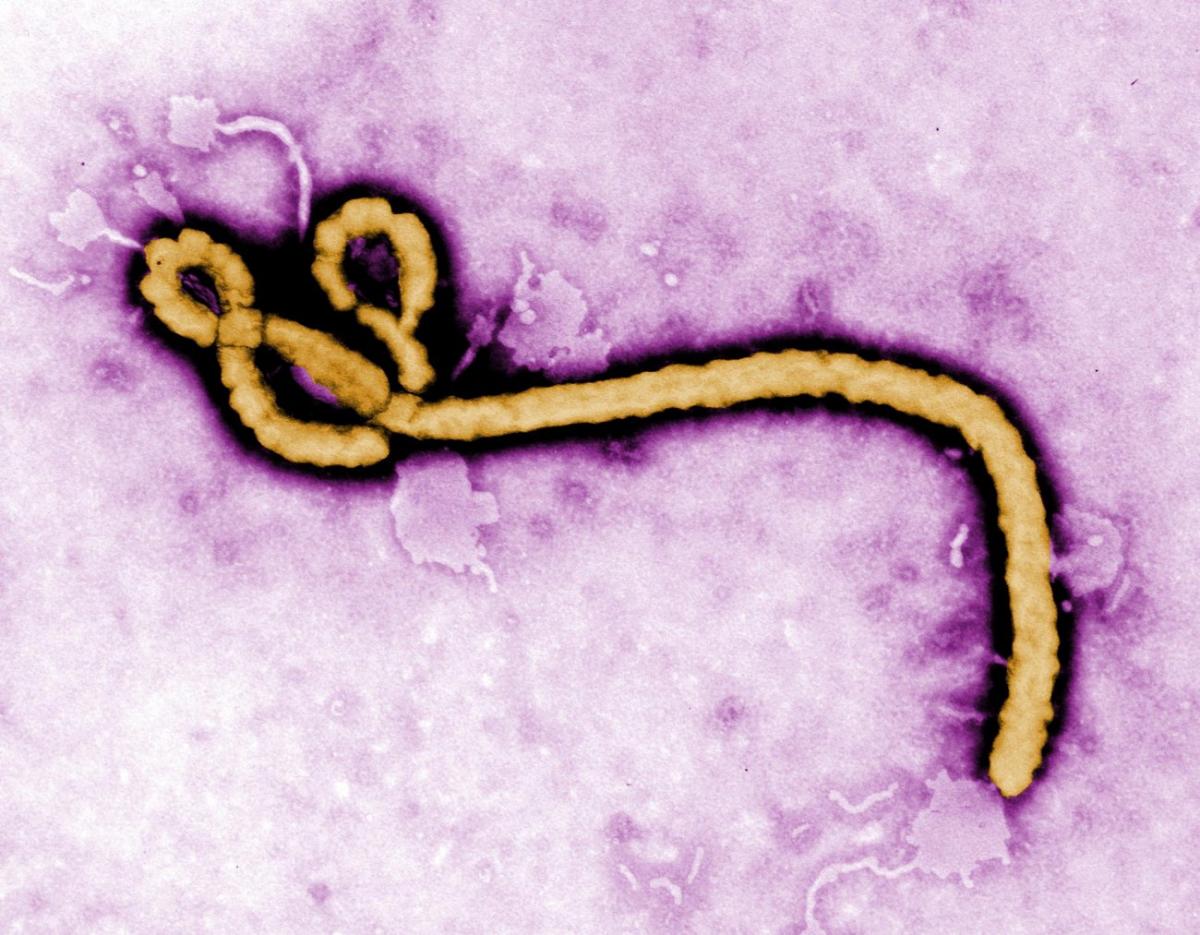
 NSAID / Flickr
NSAID / Flickr

 Boston University scientists curbed the host response to Ebola infection by inhibiting TLR4 in macrophages. (CDC Global CC BY 2.0)
Boston University scientists curbed the host response to Ebola infection by inhibiting TLR4 in macrophages. (CDC Global CC BY 2.0)


Recent Comments